Hip Innovation Technology Advances Reverse Hip Replacement System
February 9, 2023 – OrthoSpineNews –
- What are some of the shortcomings of current Total Hip Arthroplasty?
Total Hip Arthroplasty (THA) was introduced in the late 1950s by the innovative surgeon John Charnley, MD. Since that time, only minor incremental improvements in THA device concepts and refinements have been made. 
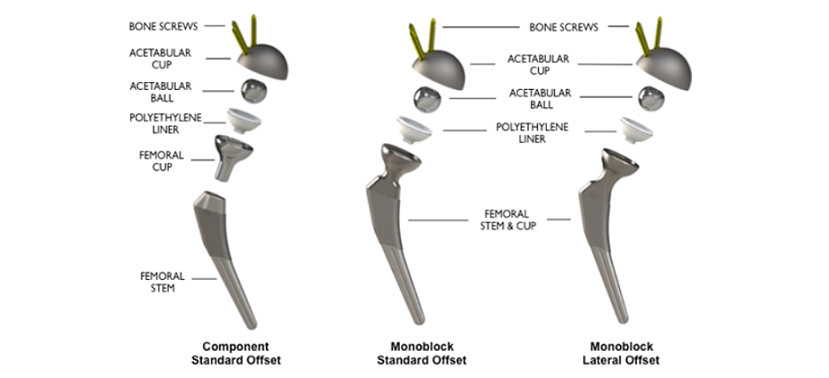
While numerous Hip Implant Systems are available, all possess the same functional designs with minimal differentiation. All systems maintain a femoral stem with an attached ball and an acetabular cup component.
Although skilled surgeons have optimized existing Hip Implant System offerings, significant challenges associated with THA remain. Primary complications are instability and dislocation, component positioning / placement and edge loading. Unfortunately, all these potential THA complications can be serious.
The most significant THA complications causing the greatest physician concern, increased health care costs and reduced patient satisfaction are dislocation and instability. Certain component positions can cause the ball of the hip prosthesis to sublux and/or dislocate. To avoid this, patients are sometimes advised after surgery not to bend more than 90 degrees at the hip and to not let their leg cross the midline of the body. The risk for dislocation is greatest in the first few months after surgery while the tissues are healing.
Accurate positioning of implant components during total hip arthroplasty is a challenging and critical step in hip replacement. Placement of the acetabular cup is of immense importance since nearly every deviation from the ideal center of rotation negatively influences endoprosthesis survival, polyethylene wear and hip load. Unfortunately, malposition of acetabular cups is quite common. In some cases, it may be unavoidable due to anatomical limitations that can affect cup placement (e.g. hip dysplasia, obesity, etc.).
Edge loading is a chiseling effect that can occur when the ball of the implant presses on the socket edge. Edge loading is associated with acetabular cup malposition and may cause accelerated component wear and increased debris particles that heighten the likelihood of osteolysis and subsequent loosening and failure of the implant.
- How does the Reverse Hip Replacement System (Reverse HRS) overcome the challenges of traditional THA?
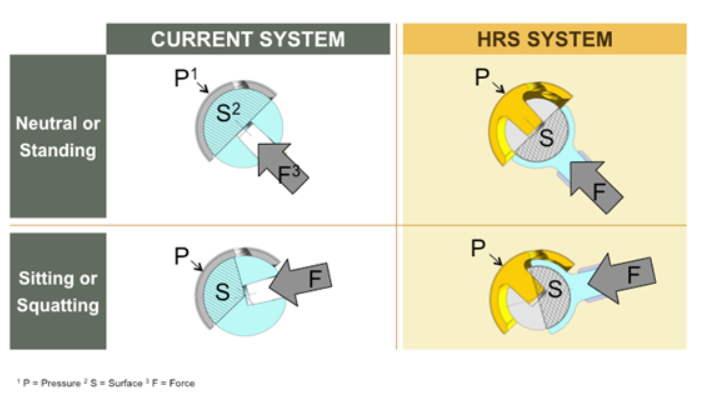
The Hip Innovation Technology (HIT) Reverse Hip Replacement System (Reverse HRS) possesses unique design features that may reduce or potentially eliminate common complications associated with THA. The Reverse HRS is a unique hip implant design that the company believes represents breakthrough technology and a significant advancement for THA.
The Reverse HRS is a unique hip implant design that possesses a ball at the center of the acetabular cup, which articulates with a femoral cup attached to the femoral stem. During motion, the edge of the femoral cup will interlock in the space situated between the acetabular ball and the acetabular cup. The Reverse HRS can be implanted in accordance with current surgical technique, to be compatible with posterior, lateral or anterior approaches and to provide a greater degree of latitude for placement of hip components relative to current designs.
- Who invented this technology?
Zafer Termanini, MD, an orthopedic surgeon, invented and designed the HIT Reverse Hip Replacement System (Reverse HRS).
- What stage of development is Reverse HRS?
Hip Innovation Technology, has initiated its pivotal Investigational Device Exemption (IDE) clinical study to evaluate the Reverse HRS in primary total hip arthroplasty (THA). This study has started and is currently enrolling patients.
- If available, will all THA patients be candidates for Reverse HRS? Or is this option only for certain patients?
The Reverse HRS is designed for use in all patients who are eligible for THA. The Reverser HRS allows forgiving placement of the acetabular cup which means patients suffering from spinal-pelvis disorders may be ideally suited for this reverse design.